First, here's a view of a typical night at the PGH Emergency Room--- where most of the action takes place.

Kinda looks like a marketplace with all those people. It's not always that hectic though---at times, patients come one at a time. There are even miraculous times when no patients come at all--- though those instances can probably be counted with the fingers of one hand. hehe. It doesn't help that whenever a Filipino patient has financial difficulties, PGH is the first hospital that comes to his mind. We have a lot of patients coming from as far as Mindanao! Due to the lack of room and equipment, we often have to turn patients away, referring them to other government hospitals where they can be given the medical treatment that they need. That's why the triage area is very vital in PGH--- and often, that area is the scene of many dramatic, sometimes violent encounters between the triage officer and patients wanting to get in. It's a sad fact that we have to turn patients away, especially if they came from some far away province, or if it's evident that they can't afford the expenses at other hospitals... but it's something that has to be done. If we admitted everyone, those who really need treatment would be greatly decompensated. Those patients that we have to refer elsewhere can't seem to understand that fact, resulting to violent reactions. It's common to hear relatives of patients shouting they'll report as to the media. What good would that do? If there's really no room or no equipment and instruments left, they won't get admitted. We can't send admitted patients out just to accomodate them. If reporting us to the media would result to more funds for PGH, then well and good. But we all know that's not the case. At the triage area, one needs to develop a heart of steel.
Enough of that already. hehe. Here's some ER cases that I've only seen in PGH.
WARNING: this is not for the faint hearted.
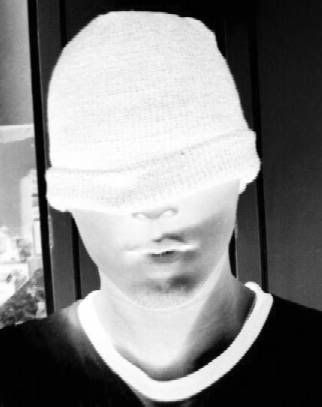
The patient pictured below has a rather peculiar history prior to his injury. You'd think it was funny actually, if you didn't see what happened to him afterwards. Few hours prior to admission, the patient was holding on to the bumper of a truck, when the truck suddenly started moving, he held on to the bumper, his face continuously in direct contact with the pavement for a few seconds while the vehicle was moving. Upon admission:

notice the extremely swollen, edematous lips. Also notice how his nose was almost falling off. As a side note, look at how relaxed he seemed, despite such massive injury. :)

There was a funny anecdote regarding this patient, I just don't know if it's true. After the patient's successful operation, he went to the out patient department after a few weeks for his scheduled follow up. The patient apparently complained that the surgeons were not able to restore his former appearance. Uhm... O--kay...
Here's a patient with a neck mass. Masses this big are rare in other hospitals since patients usually seek consult when the masses are not this large. In PGH, it's common to see patients with a 10 year history of a gradually enlarging neck mass, usually those coming from provinces. No meds. No consult. Few hours PTC, patient experienced dyspnea, thus this consult. Er--- so if he didn't experience difficulty of breathing, he won't go to a doctor at all?

This patient had a huge laceration on his neck, a result of driving a motorcycle while he was drunk--- another common mechanism of injury you'd hear while on duty at Surgery ER. Good thing he was not decapitated.

From the ER, let's move on to the Department of Pediatrics. I have a lot of pictures of pediatric patients. I mean, let's face it--- even though some people turn out to be--- er, not so good looking when they grow up, as children, most people look adorable. hehe. That's why my camera phone was extra busy during those two months, I had to buy another memory card.
I didn't really like my rotation in Pediatrics that much, because parents are so over protective of thier children. That's understandable, but it gets pretty annoying when you've been working so hard and you feel so tired and those parents can't seem to understand that what you're doing is for their children's sake. When you'll get blood from their children, which can be very difficult in Pedia patients due to their extra small veins, they get mad at you for HURTING their children. Is it too hard to understand that what you're doing is for their kid? And it's not like we're enjoying doing multiple blood extractions on their children. We actually feel bad if we don't succeed on the first try. If they don't want needles pricking their kids, why have them admitted in a hospital in the first place?! And in the pedia ER, just thinking of triage duty gives me a headache. Most of these patients are having financial difficulties, yet they go to the ER during the wee hours of the morning, during such an ungodly hour, because their child has a cold. no fever, no cough, just a cold. Only a few hours duration. I thought you'd only see that in private hospitals, wherein patients go to the ER for such trivial complaints. But no, when it comes to their children, even parents who are not financially well off develop the "PAY HOSPITAL SYNDROME". ANd many times, you'd see parents who already brought their kids to some other hospital few hours prior to consult at PGH ER, where antibiotics were already prescribed. They'd say they brought their kid to PGH because the medication is not working. D-OH! antibiotics don't work within a few hours! It's not some magic potion! You'd realize patient education is really really REALLY important.
anyway, here's one interesting case I've encountered in pedia ER. I can't remember the exact diagnosis, but if i remember correctly, our resident said the patient had an intact ethmoid sinus, so fluid was draining continuously, resulting to the malformation seen.

In the wards, there were a lot of interesting cases. A lot of babies had "big heads"--- I can't believe how many babies had hydrocephalus. My favorite patient also had a big head, but he had a different disease. I don't think I was his favorite though, because he kept crying whenever I was approaching. hehe. He had a form of brain tumor (I forgot the exact diagnosis again!). I think he already died a few months back. We sent him home because there was no more cure for his condition, it's better if he spent his last days at home. Really sad.

Here's an interesting ward case, a child with osteogenesis imperfecta. notice the flattened elbows and knees.

Here's an interesting case in the out patient department. You'd usually see people with hydrocephalus when they're still babies, and if they survive and eventually grow up, their heads are already normal sized because a shunt was already made. Imagine my surprise when this 16 year old girl walked through the door...

Sorry i can't get a better shot, a consultant was interviewing the girl. hehe.
As a pediatrics intern, we go on solo duty at the neonatal intensive care unit (NICU). Out of boredom, I took pictures of several patients. You can't help but feel pity just by looking at their condition...


One of the most exciting parts of Pediatrics rotation is the nursery duty, where babies are brought immediately after they are delivered. This is where resuscitative measures are done. Here's one baby who had four legs upon delivery. Apparently, she was supposed to be twins, but something wrong happened upon their development in the mothers womb (I'm not really in the mood for some lengthy discussion regarding the pathology, so I hope the term "wrong" would suffice. hehe).

Here's a baby with anencephaly--- born with little or no brain tissue. They usually last for only a few hours, but this baby was brought to the NICU, and although we didn't do anything, she survived for 4 whole days!

Here's another baby with anencephaly, but with more brain tissue. Also notice how she is more developed than the first baby. Her facial features are mostly developed.

When she was born, there was a new policy stating that anencephalic babies should no longer be brought to the NICU. Nothing is done to them anyway because there's no way they'll survive... unless someone's doing brain transplants these days. They'll just save the space in the NICU for babies who have a chance of surviving. So the baby was sent to her mother, at bedside. naturally, the mother freaked out--- but only initially.
OB-gyne rotation was also interesting. Here's one of my patients. She had a malignant Ovarian New Growth. Look how massive her abdomen was! Upon opening, we discovered that the ovarian growth wasn't really that big. What caused the massive abdominal enlargement was ascites. 14 liters of bloody peritoneal fluid was drained!

The patient was already weak to begin with, plus there was a lot of blood loss. The decompression of her abdomen also created problems with her blood pressure. She died a day after the operation. I remember a few minutes before anesthesia was administered, when she was still awake, she told me she wanted to get cured.SHe told me that she wanted to go to the hospital a few months back, but no one brought her until she became very weak. SHe was also seen at the OPD initially, but wasn't admitted immediately because her situation was not considered emergent at that time... And to think that was only a few days prior to her admission. She asked if she would survive. Though I did not want to give false hopes--- I knew she had a very bad prognosis--- I still said YES. I did not have the heart to tell the woman, who had such a yearning to survive, that she was, most probably--- going to die.
This is turning out to be a sad post; initially I wanted it to be a "happy", "carefree" post.... I have some more OBgyne patients, but I think those pictures are for mature audiences only.LOL. Though those pictures portray diseases, some perverted minds may still derive pleasure from them... I wouldn't want to turn this blog into a porn blog. hehe.








No comments:
Post a Comment